Shock (circulatory)
| Shock | |
|---|---|
| Classification and external resources | |
| ICD-10 | many incl. R57. |
| ICD-9 | 785 |
| DiseasesDB | 12013 |
| MedlinePlus | 000039 |
| eMedicine | emerg/531 med/285 emerg/533 |
| MeSH | D012769 |
Circulatory shock, commonly known simply as shock, is a serious, life-threatening medical condition defined as an insufficient tecidual perfusion, leading to a point at which it is inadequate to meet cellular metabolic needs. As the blood carries oxygen and nutrients around the body, reduced flow hinders the delivery of these components to the tissues, and can stop the tissues from functioning properly.[1] The process of blood entering the tissues is called perfusion, so when perfusion is not occurring properly this is called a hypoperfusional (hypo = below) state.
A circulatory shock should not be confused with the emotional state of shock, as the two are not related. Medical shock is a life-threatening medical emergency and one of the most common causes of death for critically ill people. Shock can have a variety of effects, all with similar outcomes, but all relate to a problem with the body's circulatory system. For example, shock may lead to hypoxemia (a lack of oxygen in arterial blood) or cardiac arrest (the heart stopping).[2][3][4][5][6][7][8]
The essential signs of shock are seen as tachycardia/tachypnoea (compensatory mechanisms), hypotension, and signs of poor end-organ perfusion (such as low urine output, confusion or loss of consciousness) (failure to compensate). Other signs should be looked for to establish the underlying cause for the shock to guide effective treatment.
Contents |
Signs of severity
The severity of shock can be graded 1-4 based on the physical signs. This approximates to the effective loss of blood volume. The blood volume does not have to actually be lost from the circulation as an expansion in the volume of the circulatory system (e.g. in septic shock) will render the patient proportionally hypovolaemic.
- Grade 1
- Up to about 15% loss of effective blood volume (~750ml in an average adult who is assumed to have a blood volume of 5 liters). This leads to a mild resting tachycardia and can be well tolerated in otherwise healthy individuals. In the elderly or those with underlying conditions such as ischaemic heart disease the additional myocardial oxygen demands may not be tolerated so well.
- Grade 2
- Between 15-30% loss of blood volume (750-1500ml) will provoke a moderate tachycardia and begin to narrow the pulse pressure. The time taken for the capillaries to refill after 5 seconds of pressure (capillary refill time) will be extended.
- Grade 3
- At 30 - 40% loss of effective blood volume (1500 - 2000 ml) the compensatory mechanisms begin to fail and hypotension, tachycardia and low urine output (<0.5ml/kg/hr in adults) are seen.
- Grade 4
- At 40-50% loss of blood volume (2000 -2500 ml) profound hypotension will develop and if prolonged will cause end-organ damage and death.
Signs relating to different causes
- Hypovolaemic shock
- Direct loss of effective circulating blood volume leading to:
- Anxiety, restlessness, altered mental state due to decreased cerebral perfusion and subsequent hypoxia
- Hypotension due to decrease in circulatory volume
- A rapid, weak, thready pulse due to decreased blood flow combined with tachycardia
- Cool, clammy skin due to vasoconstriction and stimulation of vasoconstriction
- Rapid and shallow respirations due to sympathetic nervous system stimulation and acidosis
- Hypothermia due to decreased perfusion and evaporation of sweat
- Thirst and dry mouth, due to fluid depletion
- Fatigue due to inadequate oxygenation
- Cold and mottled skin (cutis marmorata), especially extremities, due to insufficient perfusion of the skin
- Distracted look in the eyes or staring into space, often with pupils dilated
- Cardiogenic shock
- Similar to hypovolemic shock but in addition:
- Distended jugular veins due to increased jugular venous pressure
- Weak or absent pulse
- Arrhythmia, often tachycardic
- Obstructive shock
- Similar to hypovolemic shock but in addition:
- Distended jugular veins due to increased jugular venous pressure
- Pulsus paradoxus in case of tamponade
- Septic shock
- Similar to hypovolemic shock except in the first stages:
- Pyrexia (fever), due to increased level of cytokines[1]
- Systemic vasodilation resulting in hypotension (low blood pressure)[1]
- Warm and sweaty skin due to vasodilation
- Systemic leukocyte adhesion to endothelial tissue[1]
- Reduced contractility of the heart[1]
- Activation of the coagulation pathways, resulting in disseminated intravascular coagulation[1]
- Increased levels of neutrophils[1]
- Neurogenic shock
- As with hypovolemic shock but in high spinal injuries may also be accompanied by profound bradycardia due to loss of the cardiac accelerating nerve fibres from the sympathetic nervous system at T1-T4.
- The skin is warm and dry or a clear sweat line exists, above which the skin is diaphoretic.
- Priapism due to Peripheral nervous system stimulation
- Anaphylactic shock
- Skin eruptions and large bumps
- Localised oedema, especially around the face
- Weak and rapid pulse
- Breathlessness and cough due to narrowing of airways and swelling of the throat
Pathophysiology
There are four stages of shock. As it is a complex and continuous condition there is no sudden transition from one stage to the next.[9]
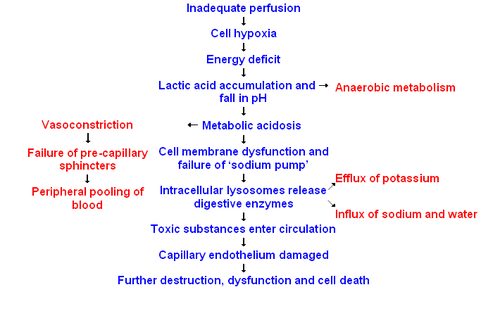
- Initial
- During this stage, the hypoperfusional state causes hypoxia, leading to the mitochondria being unable to produce adenosine triphosphate (ATP). Due to this lack of oxygen, the cell membranes become damaged, they become leaky to extra-cellular fluid, and the cells perform anaerobic respiration. This causes a build-up of lactic and pyruvic acid which results in systemic metabolic acidosis. The process of removing these compounds from the cells by the liver requires oxygen, which is absent.
- Compensatory (Compensating)
- This stage is characterised by the body employing physiological mechanisms, including neural, hormonal and bio-chemical mechanisms in an attempt to reverse the condition. As a result of the acidosis, the person will begin to hyperventilate in order to rid the body of carbon dioxide (CO2). CO2 indirectly acts to acidify the blood and by removing it the body is attempting to raise the pH of the blood. The baroreceptors in the arteries detect the resulting hypotension, and cause the release of adrenaline and noradrenaline. Noradrenaline causes predominately vasoconstriction with a mild increase in heart rate, whereas adrenaline predominately causes an increase in heart rate with a small effect on the vascular tone; the combined effect results in an increase in blood pressure. This is known as Cushing reflex and its triad is the subjective identifying characteristic of this stage. Renin-angiotensin axis is activated and arginine vasopressin (Anti-diuretic hormone; ADH) is released to conserve fluid via the kidneys. Also, these hormones cause the vasoconstriction of the kidneys, gastrointestinal tract, and other organs to divert blood to the heart, lungs and brain. The lack of blood to the renal system causes the characteristic low urine production. However the effects of the Renin-angiotensin axis take time and are of little importance to the immediate homeostatic mediation of shock .
- Progressive (Decompensating)
- Should the cause of the crisis not be successfully treated, the shock will proceed to the progressive stage and the compensatory mechanisms begin to fail. Due to the decreased perfusion of the cells, sodium ions build up within while potassium ions leak out. As anaerobic metabolism continues, increasing the body's metabolic acidosis, the arteriolar smooth muscle and precapillary sphincters relax such that blood remains in the capillaries[1]. Due to this, the hydrostatic pressure will increase and, combined with histamine release, this will lead to leakage of fluid and protein into the surrounding tissues. As this fluid is lost, the blood concentration and viscosity increase, causing sludging of the micro-circulation. The prolonged vasoconstriction will also cause the vital organs to be compromised due to reduced perfusion[1]. If the bowel becomes sufficiently ischemic, bacteria may enter the blood stream, resulting in the increased complication of endotoxic shock[1].
- Refractory (Irreversible)
- At this stage, the vital organs have failed and the shock can no longer be reversed. Brain damage and cell death have occurred. Death will occur imminently.
Types
Hinshaw and Cox classification
In 1972 Hinshaw and Cox suggested the following classification which is still used today.[2] It names four types of shock: hypovolemic, cardiogenic, distributive and obstructive shock:[3][4][5][8][10] In many patients, shock is a combination of two or more of these four types of shock.
Hypovolemic shock
This is the most common type of shock and based on insufficient circulating volume. Its primary cause is loss of fluid from the circulation (most often "hemorrhagic shock"). Causes may include internal bleeding, traumatic bleeding, high output fistulae or severe burns.
Cardiogenic shock
This type of shock is caused by the failure of the heart to pump effectively. This can be due to damage to the heart muscle, most often from a large myocardial infarction. Other causes of cardiogenic shock include arrhythmias, cardiomyopathy, congestive heart failure (CHF), contusio cordis, or cardiac valve problems.
Distributive shock
As in hypovolaemic shock there is an insufficient intravascular volume of blood. This form of "relative" hypovolaemia is the result of dilation of blood vessels which diminishes systemic vascular resistance. Examples of this form of shock are:
- Septic shock
- Caused by an overwhelming systemic infection resulting in vasodilation leading to hypotension. Septic shock can be caused by Gram negative bacteria such as (among others) Escherichia coli, Proteus species, Klebsiella pneumoniae which release an endotoxin which produces adverse biochemical, immunological and occasionally neurological effects which are harmful to the body, and other Gram-positive cocci, such as pneumococci and streptococci, and certain fungi as well as Gram-positive bacterial toxins. Septic shock also includes some elements of cardiogenic shock. In 1992, the ACCP/SCCM Consensus Conference Committee defined septic shock: ". . .sepsis-induced hypotension (systolic blood pressure <90 mm Hg or a reduction of 40 mm Hg from baseline) despite adequate fluid resuscitation along with the presence of perfusion abnormalities that may include, but are not limited to, lactic acidosis, oliguria, or an acute alteration in mental status. Patients who are receiving inotropic or vasopressor agents may have a normalized blood pressure at the time that perfusion abnormalities are identified."
- Anaphylactic shock
- Caused by a severe anaphylactic reaction to an allergen, antigen, drug or foreign protein causing the release of histamine which causes widespread vasodilation, leading to hypotension and increased capillary permeability.
- Neurogenic shock
- Neurogenic shock is the rarest form of shock. It is caused by trauma to the spinal cord resulting in the sudden loss of autonomic and motor reflexes below the injury level. Without stimulation by sympathetic nervous system the vessel walls relax uncontrollably, resulting in a sudden decrease in peripheral vascular resistance, leading to vasodilation and hypotension. (This term can be confused with Spinal shock which is a recoverable loss of function of the spinal cord after injury and does not refer to the haemodynamic instability per se.)
Obstructive shock
In this situation the flow of blood is obstructed which impedes circulation and can result in circulatory arrest. Several conditions result in this form of shock.
- Cardiac tamponade
- in which fluid in the pericardium prevents inflow of blood into the heart (venous return). Constrictive pericarditis, in which the pericardium shrinks and hardens, is similar in presentation.
- Tension pneumothorax
- Through increased intrathoracic pressure, bloodflow to the heart is prevented (venous return).
- Massive pulmonary embolism
- is the result of a thromboembolic incident in the bloodvessels of the lungs and hinders the return of blood to the heart.
- Aortic stenosis
- hinders circulation by obstructing the ventricular outflow tract
Other proposed types of shock
Revisions to the Hinshaw and Cox classification have been proposed. Several types of shock have been proposed as a "fifth type of shock", including hypoglycemic shock, cytotoxic shock and endocrine shock. However, each of these is actually a subtype of one of the four types of shock in Hinshaw and Cox's original model.
For example:
- Endocrine shock
- Based on endocrine disturbances such as:
- Hypothyroidism (Can be considered a form of Cardiogenic shock)
- in critically ill patients, reduces cardiac output and can lead to hypotension and respiratory insufficiency.
- Thyrotoxicosis (Cardiogenic shock)
- may induce a reversible cardiomyopathy.
- Acute adrenal insufficiency (Distributive shock)
- is frequently the result of discontinuing corticosteroid treatment without tapering the dosage. However, surgery and intercurrent disease in patients on corticosteroid therapy without adjusting the dosage to accommodate for increased requirements may also result in this condition.
- Relative adrenal insufficiency (Distributive shock)
- in critically ill patients where present hormone levels are insufficient to meet the higher demands
Treatment
Shock requires immediate interventions to preserve life. Therefore, the early recognition and treatment is essential even before a specific diagnosis is made (As a general rule, you should treat for a sustained wound and shock). Most forms of shock seen in trauma or sepsis respond initially to aggressive intravenous fluids (e.g. 1 liter normal saline bolus over 10 minutes or 20ml/kg in a child). Therefore this treatment is usually instituted as the person is being further evaluated.[11]
Re-establishing perfusion to the organs is the primary goal through restoring and maintaining the blood circulating volume ensuring oxygenation and blood pressure are adequate, achieving and maintaining effective cardiac function, and preventing complications. Patients attending with the symptoms of shock will have, regardless of the type of shock, their airway managed and oxygen therapy initiated. In case of respiratory insufficiency (i.e. diminished levels of consciousness, hyperventilation due to acid-base disturbances or pneumonia) tracheal intubation and mechanical ventilation may be necessary. A paramedic may intubate in emergencies outside the hospital, whereas a patient with respiratory insufficiency in-hospital will be intubated usually by a respiratory therapist, paramedic, or physician.
The aim of these acts is to ensure survival during the transportation to the hospital; they do not cure the cause of the shock. Specific treatment depends on the cause.
Prognosis
The prognosis of shock depends on the underlying cause and the nature and extent of concurrent problems. Hypovolemic, anaphylactic and neurogenic shock are readily treatable and respond well to medical therapy. Septic shock however, is a grave condition and with a mortality rate between 30% and 50%. The prognosis of cardiogenic shock is even worse.[2]
Shock is said to evolve from reversible to irreversible in experimental hemorrhagic shock involving certain animal species (dogs, rats, mice) that develop intense vasoconstriction of the gut. Death is due to hemorrhagic necrosis of the intestinal lining when shed blood in reinfused. In pigs and humans 1) this is not seen and cessation of bleeding and restoration of blood volume is usually very effective; however 2) prolonged hypovolemia and hypotension does carry a risk of respiratory and then cardiac arrest. Perfusion of the brain may be the greatest danger during shock. Therefore urgent treatment (cessation of bleeding, rapid restoration of circulating blood volume and ready respiratory support) is essential for a good prognosis in hypovolemic shock.
See also
- Acute respiratory distress syndrome (ARDS)
- Anaesthesia Trauma and Critical Care
- Non-pneumatic anti-shock garment
- Physical trauma
- Sepsis
- Stress (medicine)
- Systemic inflammatory response syndrome (SIRS)
References
- ↑ 1.0 1.1 1.2 1.3 1.4 1.5 1.6 1.7 1.8 1.9 Kumar, Vinay; Abbas, Abul K.; Fausto, Nelson; & Mitchell, Richard N. (2007). Robbins Basic Pathology (8th ed.). Saunders Elsevier. pp. 102-103 ISBN 978-1-4160-2973-1
- ↑ 2.0 2.1 2.2 Irwin, Richard S.; Rippe, James M. (January 2003). Intensive Care Medicine. Lippincott Williams & Wilkins, Philadelphia & London. ISBN 0-7817-3548-3.
- ↑ 3.0 3.1 Marino, Paul L. (September 2006). The ICU Book. Lippincott Williams & Wilkins, Philadelphia & London. ISBN 0-7817-4802-X.
- ↑ 4.0 4.1 "Fundamental Critical Care Support, A standardized curriculum of Critical Care". Society of Critical Care Medicine, Des Plaines, Illinois. http://www.sccm.org/SCCM/FCCS+and+Training+Courses/FCCS/FCCSCourseAdmin.htm.
- ↑ 5.0 5.1 Harrison's Principles of Internal Medicine. http://books.mcgraw-hill.com/medical/harrisons/.
- ↑ "Cecil Textbook of Medicine". http://www.cecilmedicine.com/buy.cfm?book=goldman.
- ↑ The Oxford Textbook of Medicine. http://www.oup.com/us/catalog/general/subject/Medicine/PrimaryCare/?ci=0192629220&view=usa.
- ↑ 8.0 8.1 Shock: An Overview PDF by Michael L. Cheatham, MD, Ernest F.J. Block, MD, Howard G. Smith, MD, John T. Promes, MD, Surgical Critical Care Service, Department of Surgical Education, Orlando Regional Medical Center Orlando, Florida
- ↑ Armstrong, D.J. (2004). Shock. In: Alexander, M.F., Fawcett, J.N., Runciman, P.J. Nursing Practice. Hospital and Home. The Adult.(2nd edition): Edinburgh: Churchill Livingstone.
- ↑ Joynt, Gavin (April 2003). "Introduction to management of shock for junior ICU trainees and medical students". The Chinese University of Hong Kong. http://www.aic.cuhk.edu.hk/web8/shock.htm. Retrieved 9 October 2006.
- ↑ American College of Surgeons (2008). Atls, Advanced Trauma Life Support Program for Doctors. Amer College of Surgeons. pp. 58. ISBN 1-880696-31-6.
|
||||||||||||||||||||||||||||||||||
|
||||||||||||||||||||||||||||||||||||||||||